Diabetes mellitus causes numerous vision problems such as: changes in refraction, elevated intraocular pressure, cataract. However, the most common condition is diabetic retinopathy, which occurs in more than 85% of people with diabetes and represents one of the most serious complications of diabetes.
How does diabetic retinopathy develop?
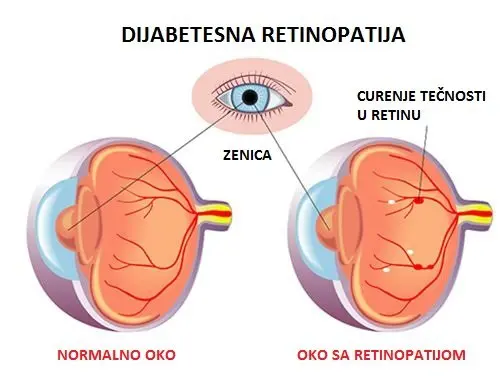
Diabetes damages the blood vessels in the eye, preventing proper blood supply and adequate nourishment of the retina. As a consequence of poor circulation in the eye due to long-standing and inadequately treated diabetes, new pathological blood vessels of poorer quality are formed, with thin, fragile walls that easily rupture and leak blood into the surrounding tissue.
All of this results in the accumulation of fluid and blood in the area of the macula (the point of sharp vision) – diabetic macular edema, which leads to a decrease in vision. In the later stages of the disease, the patient loses vision due to bleeding into the vitreous body, and retinal detachment may also occur, as well as secondary glaucoma.
The diagnosis is made precisely and accurately by examining the fundus with dilated pupils, as well as with the help of OCT (optical coherence tomography). In the case of macular edema, it is sometimes necessary to perform fluorescein angiography (imaging of the fundus blood vessels using contrast). In the case of dense cataract and bleeding into the vitreous body – hemophthalmos, it is necessary to assess the condition of the retina by ultrasound.
OCT of the eyeUltrasound examination of the eye
Symptoms of diabetic retinopathy
Unfortunately, diabetic retinopathy has no pronounced symptoms until the advanced stage of the disease (proliferative diabetic retinopathy). Changes can progress for a long time without being noticed and cause significant visual damage due to bleeding. If the disease is not detected and treated in time, it leads to permanent loss of vision, i.e. blindness.
It is therefore important to emphasize the need for regular fundus examinations in patients with diabetes, so that treatment can begin as early as possible.
Some of the first symptoms a patient may notice are a decrease in visual acuity and distorted images (due to diabetic retinopathy), but also a sudden loss of vision (due to bleeding into the vitreous body), which patients notice as a moving curtain or a spot floating in the eye. The occurrence of such symptoms requires an urgent visit to an ophthalmologist.
Treatment of diabetic retinopathy
The treatment of diabetic retinopathy is complex and long-term, and the longer treatment is delayed, the harder it is to achieve a satisfactory result.
The disease is treated, depending on how dense the bleeding is, in three ways:
We use laser photocoagulation as a treatment for diabetic edema – swelling of the macula, as well as in proliferative diabetic retinopathy (the final stage of the disease in which the eye tries to compensate for insufficient nourishment by forming new pathological blood vessels that bleed and thus cause the patient to lose vision). With this laser treatment, it is possible to slow down or, in the best case, stop the deterioration of vision in people with diabetes.
This is a painless, outpatient procedure performed under topical anesthesia in the form of eye drops, using a contact lens placed on the patient’s eye. The patient sees flashes of green laser light entering the eye through the lens. The procedure lasts about 10 minutes, and for a few minutes afterwards vision is reduced, similar to the feeling after being photographed with a strong flash. After the treatment, the patient goes home with a recommendation to use anti-inflammatory therapy (eye drops) for the next 4 weeks.
Injection of anti-VEGF into the eye
Today, the recommendation is that after diagnosing a pronounced macular edema, before laser treatment, medications are applied directly into the eye – intravitreal injections of drugs that are inhibitors of vascular endothelial growth factor – anti-VEGF therapy.
These drugs stabilize the blood vessels and, on the one hand, help the edema to be absorbed, and on the other hand prevent the spread of pathological blood vessels. The goal is to reduce the swelling as much as possible with a few doses of these drugs, so that a laser of the lowest possible power can be applied, and therefore less destructive to such valuable tissue as the macula, i.e. the point of sharp vision.
Injection into the eyeInjection into the eyeInjection into the eye
After anesthetizing the eye with a local anesthetic given in the form of drops, the medication is injected into the vitreous cavity of the eye (the “gel” that fills three-quarters of our eye). The procedure is painless. It is recommended that the application be performed in an operating room, under sterile conditions, by a trained surgeon – a retinal specialist. The treatment is repeated at intervals of 4 to 6 weeks, depending on the achieved effect.
Vitrectomy
This very complex surgery is the final stage of treatment and is used in the advanced stage of proliferative diabetic retinopathy. Unfortunately, with this operation the goal is most often to preserve functional visual acuity, as more significant improvements cannot be achieved.
During the surgery, the vitreous body filled with blood is removed and replaced with a clear solution (silicone oil) or gas, which allows the retina to remain in place, attached to the layers of the eye beneath it.
It is important that vitreoretinal surgery is performed in a timely manner, because deformation or detachment of the retina can be devastating for vision.
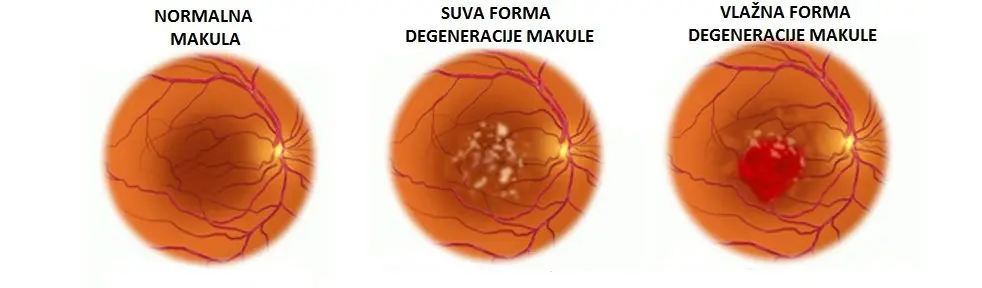
Types of macular degeneration
Dry form of macular degeneration represents the initial stage of the disease and occurs in about 85% of cases. It is a consequence of the gradual degeneration of the photosensitive cells of the macula. This form of the disease progresses very slowly, so the patient does not notice visual disturbances for a long time. Central vision gradually weakens, which manifests as: difficulty reading, difficulty perceiving details, and the appearance of a spot in the center of the visual field.
Wet form of macular degeneration represents a more severe form of the disease and occurs in about 15% of cases. Central vision deteriorates rapidly and, due to fluid leakage from fragile newly formed blood vessels, the patient experiences early symptoms such as the appearance of wavy lines and distortion of object contours. If the disease is allowed to follow its natural course, there is increasing fluid leakage and bleeding, and eventually complete destruction of the macula occurs, with scar formation resulting in permanent and severe visual impairment.
The appearance of wavy lines is an important symptom indicating that the patient should see an ophthalmologist for a detailed fundus examination. An irreplaceable role in diagnosis and monitoring of the disease is played by OCT (optical coherence tomography), as a non-invasive and rapid method of assessing the condition of the macula. Another important diagnostic tool is FA (fluorescein angiography).
At-risk groups include: people over 60 years of age, relatives of affected individuals, women, people with poorly controlled hypertension, smokers, and obese individuals.
Treatment of macular degeneration
It is considered that the use of certain antioxidants can slow the progression to the advanced form of macular degeneration. Patients who come regularly for check-ups, if they show signs of disease progression, are instructed and given an Amsler grid, with which they periodically test their central vision. If they notice that lines are starting to become distorted, it is necessary to see an ophthalmologist urgently in order to begin diagnostic and therapeutic procedures.
Treatment with anti-VEGF drugs (Eylea, Avastin) is used in the wet form of macular degeneration.
An elevated level of growth factors in the affected eye stimulates the growth of new fragile blood vessels. This injection blocks the growth factors and thus slows and blocks the growth of fragile blood vessels, which slows the deterioration of vision.
It is given under local anesthesia, so the patient does not feel pain, and after a short observation period, the patient goes home with a bandage that is removed upon arrival home.
To maintain the effect of therapy, the injection must be repeated at certain time intervals. A better effect is achieved if the changes are not advanced, but it is important to emphasize that no drug has yet been found that could cure this condition.
Laser treatment involves destroying fragile newly formed blood vessels and is performed in a smaller number of cases, when these vessels are located outside the fovea (the central part of the macula). After treatment, new growth of blood vessels and the need for retreatment are possible.
Find answers to the most common questions about laser vision correction, cataracts and lens implantation. Everything you need to know before deciding on a procedure.
No, the procedure is completely painless. It takes only a few minutes, and as early as the next day you can function normally without glasses or lenses.
If you notice that your vision is blurry, colors are fading and you struggle to drive at night, these are clear warning signs. Surgery restores clear vision and once cataracts are diagnosed, it should not be postponed.
The biggest advantage is that you forget about glasses – both for near and far. This means you can read a book, use your phone and drive without additional visual aids.
You absolutely do! Toric lenses are specifically designed to correct astigmatism and provide clear vision.
These are artificial lenses that are placed inside the eye, while your natural lens remains untouched. They are an excellent option for younger people with high diopters who are not candidates for laser vision correction.